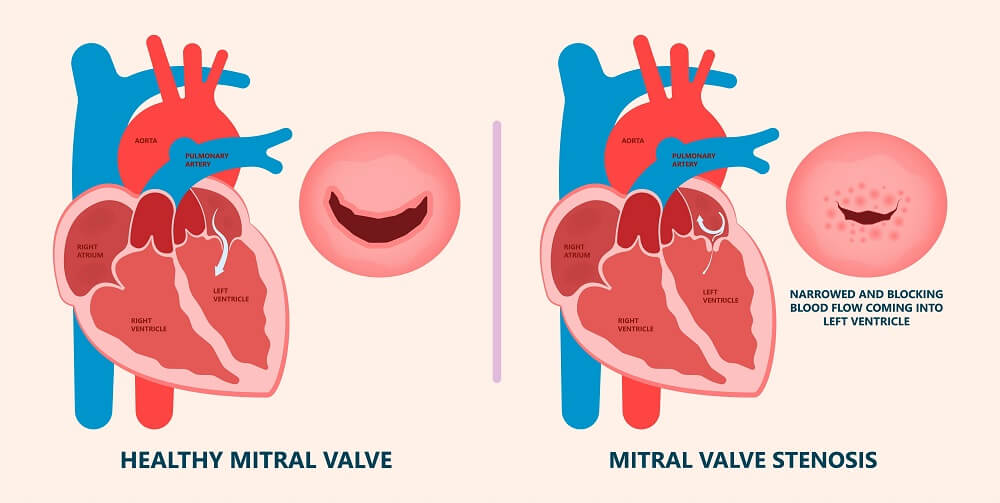
Mitral Valve is the one which is tucked between the upper left atrium and lower left ventricle and when it gets narrowed, this becomes a major heart health issue which is called Mitral Valve Stenosis. Under this condition, the blood flow from the left atrium to the left ventricle is restricted and the blood starts to flow back into the left atrium, blood vessels of the lungs and to the right side of the heart too. Though stenosis occurs, symptoms don’t appear for a major part of one’s life, say 8 to 10 years. But in India, research suggests that the progression is quicker than in the rest of the world and symptoms surface within 8 to 10 years. As for the severity, such can be mild or severe. What are the possible reasons for mitral valve stenosis that we know? Notable Symptoms Of Mitral Valve Stenosis: III. Cough. VII. Swelling in leg, feet and ankles. VIII. Heart rhythms get abnormal. What are the difficulties that arise from Mitral Valve stenosis? The following issues have come to light. This is called heart enlargement where the upper left chamber (left atrium) gets bigger in size and the right side of the heart which is due to pressure taking place as a fallout of mitral valve stenosis. Upper chambers get stretched and get bigger and this often leads to strange heart rhythm. If we ignore abnormal or ultrafast heartbeats, we find blood clots in the left atrium. Further, such clots can split and travel to different parts of the body and this gives rise to troubling consequences like paralytic stroke. Pressure increases in the upper left chamber and lungs and this gives rise to risky fluid accumulation which can also cause heart failure. Blood pressure increases in the arteries which facilitate blood flow from the heart to the lungs (pulmonary arteries). How do the doctors (the best cardiologist for valve replacement for that matter) diagnose mitral valve stenosis? This is a complication which goes unnoticed for a few years but when the stenosis progression takes place, problems appear. Doctors prescribe the following tests to detect the disease. If left untreated and ignored, the small problem can grow into a big problem (and would need more money for treatment). Smashing the boundaries, his clinic embraces cutting-edge technology and such machines help in effective and world-class treatment of a range of heart issues, at a reasonable price but still, one has to remember that no cost is high for saving a life and to lead a healthy life. As a result, Dr C Ragu’s clinic is the shining jewel of Hyderabad city as the eclectic world of Dr C Raghu’s modern cardiology enthralls everyone. We make a successful pitch for supreme heartcare and treatment excellence in India which is at par with the developed world located in the west and is more affordable too. Truly, Dr C Raghu is widely regarded as the best cardiologist for valve replacement and has a large fan following across the world.
Dr C Raghu: The Saviour Of Heart Health.
Book Online Consultaion
How Cholesterol Is Linked to Heart Disease Blog
Subscribe the Hearty Life Blogs

DR. RAGHU | Best Cardiologist in Hyderabad
Cardiology Coronary, Vascular and
Structural InterventionsConditions & Diseases
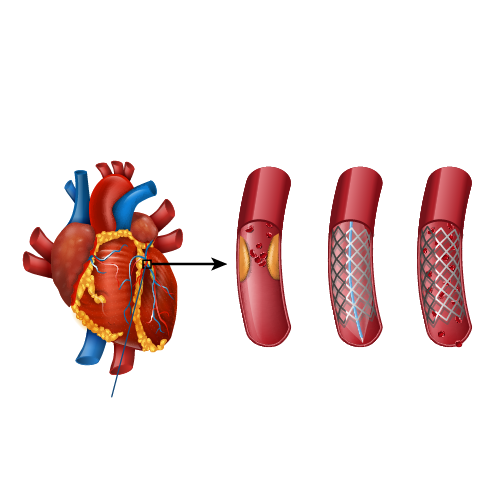
Angioplasty
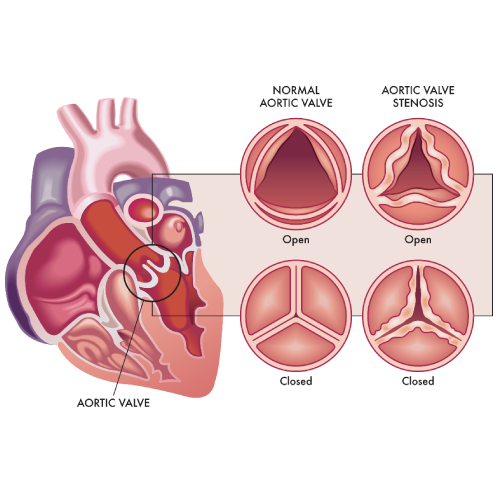
Aortic Stenosis
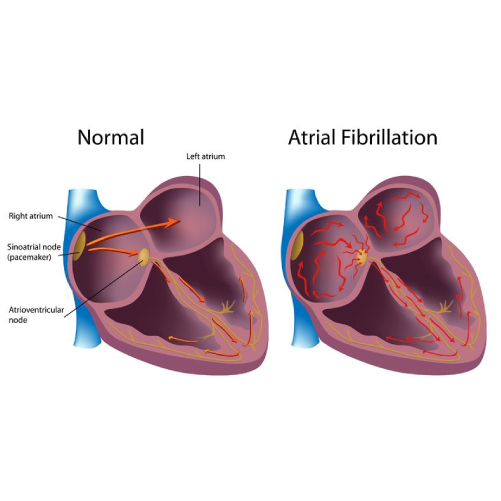
Atrial Fibrillation
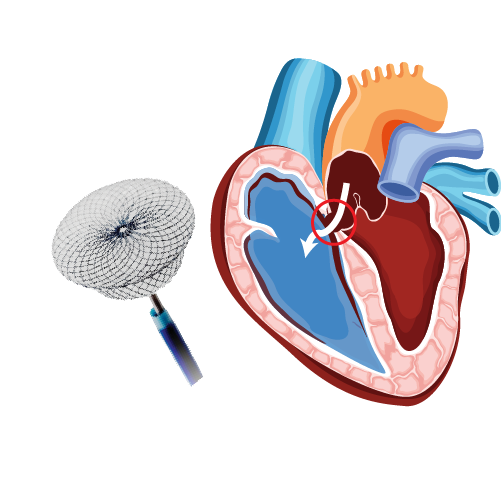
Atrial Septal Defect
Related Posts