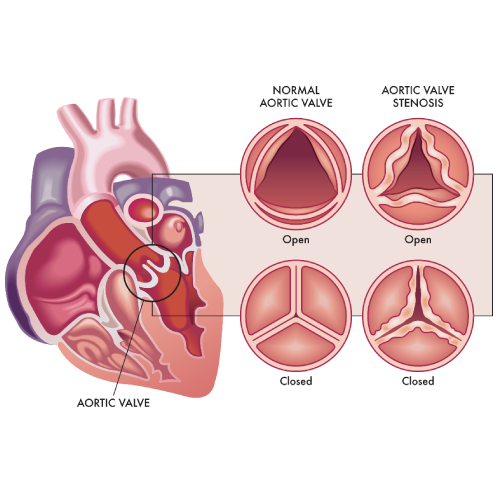
- In around 40% of aortic stenosis (AS) cases assessment of severity is discordant – area-gradient mismatch: area is smaller but pressure gradient is low or reverse area-gradient mismatch where the gradient is higher and area stenosis is less severe.1,2
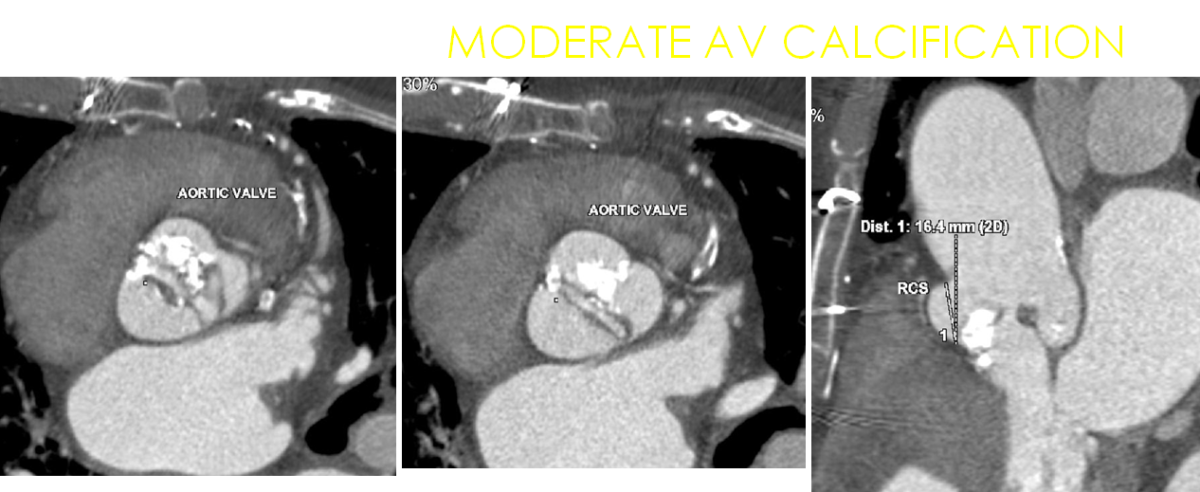
- Measurement of aortic valve calcium (AVC) is an emerging parameter in cases with discordant echocardiographic findings.
- Discordant findings are common in the elderly because they have concomitant coronary artery disease, left ventricle dysfunction and other valve lesions. This is a compelling reason to perform a multi-modality imaging for to accurately assess severity of AS who could definitely be benefitted from Transcatheter Aortic Valve Replacement (TAVR).
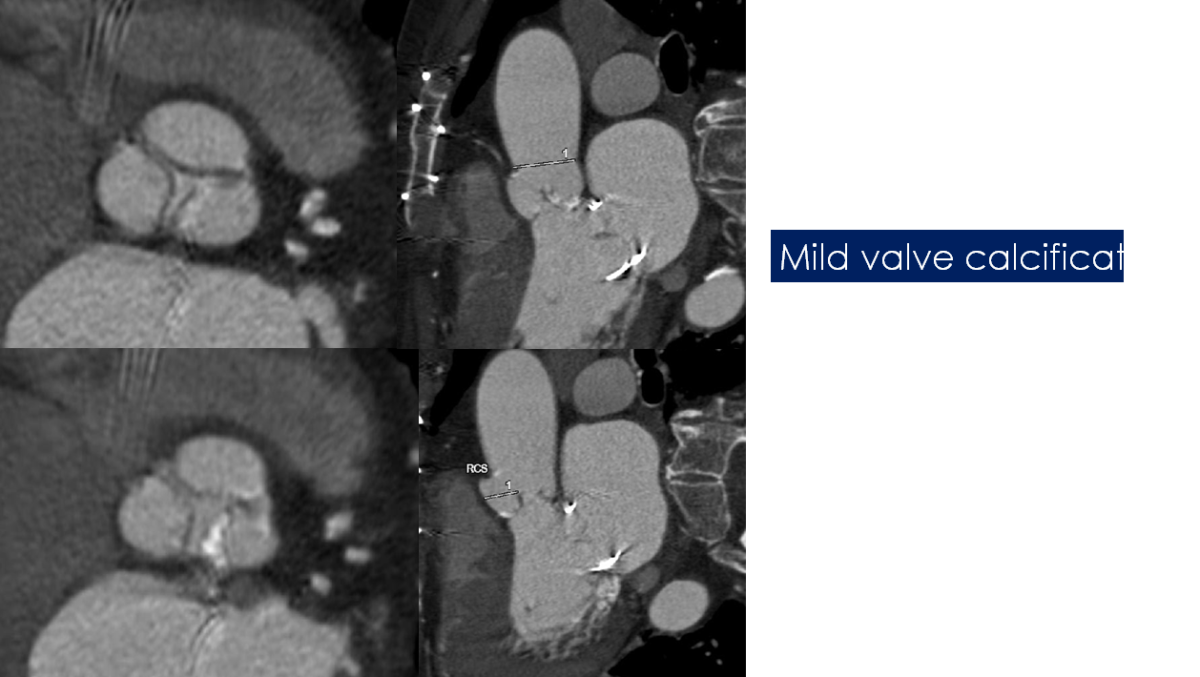
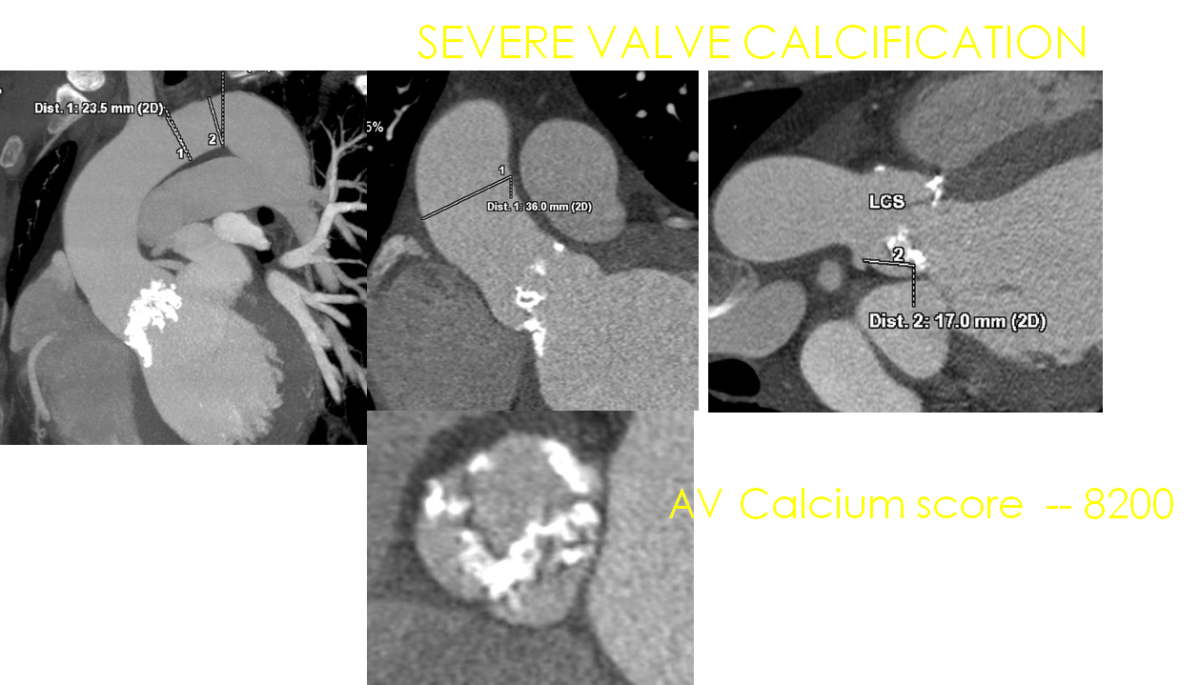
- AVC is obtained on non contrast, non ECG gated CT scan using the Agatston method.
- Assessment of AVC is a useful tool for identifying patients who may benefit from TAVR.
- Calcification of the mitral annulus, left ventricular outflow tract and coronaries should be carefully excluded from AVC measurement.
- AVC score of more than 1300 in women and 2000 in men is considered as severe AS.
- Sensitivity and specificity of this parameter are 82 and 78% respectively.
- AVC has a strong prognostic value with a hazard ratio for mortality 2.11.
- Indexation of AVC to body surface area did not add incremental prognostic value.
- CT based AVC estimation has been recommended in the latest 2017 ESC guidelines on valvular heart disease as a complementary method to estimate the severity of AS.
- The gold standard for estimation of AS severity is echocardiography and AVC is a complementary modality only.
- In patients with area:gradient mismatch AVC has an excellent diagnostic value.
- Compared to dobutamine stress echo this is a simple, faster tool. Also the risk of radiation is low.
- Patients with less severe but significant CT AVC, frequent close monitoring of AS progression is needed.
- Limitations of AVC:
- At times the AS pathology is predominantly fibrotic rather than calcific – eg. women with bicuspid aortic valve.
- Fibrotic leaflet thickening can also lead to hemodynamic obstruction that can’t be identified by AVC.

Conclusion:
Aortic valve calcification as measured by CT is an accurate, reproducible, and well-validated marker of stenosis severity, progression of disease, and a powerful predictor of adverse events.
In patients with discordant echo findings and are symptomatic estimation of AVC is a simple tool for those who benefit from TAVR or TAVI.
- Conditions
Conditions
- Acute limb ischemia
- Chronic limb ischemia
- Aortic stenosis
- Mitral valve stenosis
- Mitral valve regurgitation
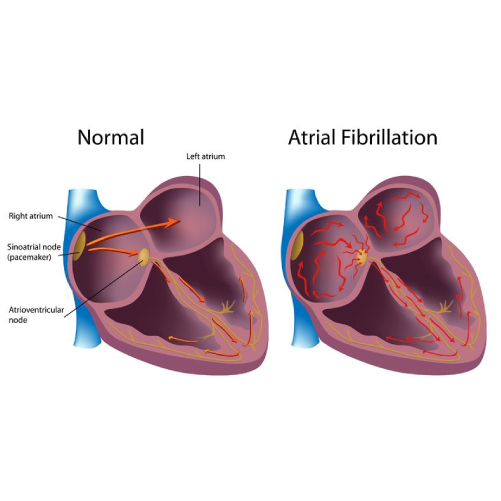
- Atrial fibrillation
- Tachycardia
- Bradycardia
- Palpitations
- High blood pressure
- Atrial septal defect
- Ventricular septal defect
- Patent ductus arteriosus
- Cardiac amyloidosis
- Hypertrophic cardiomyopathy
- Varicose veins
- Deep vein thrombosis (DVT)
- Myocarditis
- Endocarditis
- Pericarditis
- Peripheral arterial disease
- Pulmonary artery hypertension
- Pulmonary embolism
- Cath lab procedures:
Cath lab procedures:
- Coronary Angiogram
- Primary Angioplasty
- Coronary Angioplasty
- CHIP Angioplasty
- Aortic valve replacement surgery
- Mitral valve replacement surgery
- Device closure for Atrial septal defect
- Device closure for Ventricular septal defect
- Device closure for Patent Ductus Arteriosus
- Transcatheter aortic valve replacement (TAVR)
- Inferior vena cava (IVC) filter
- LA appendage closure
- Fistuloplasty
- Balloon mitral valvotomy
- 24 hours emergency services
24 hours emergency services
- Clinics- weekly basis/monthly basis/ Yearly basis
Clinics- weekly basis/monthly basis/ Yearly basis
- Prevention of cardiovascular diseases
Prevention of cardiovascular diseases
- Diagnosis
Diagnosis
BOOK AN APPOINTMENT

Dr. RAGHU
MD, DM, FESC, FACC, FSCAI
Cardiology Coronary, Vascular and
Structural Interventions
Cardiology Coronary, Vascular and
Structural Interventions
Conditions & Diseases
Angioplasty
Aortic Stenosis
Atrial Fibrillation