Coronary artery disease (CAD) kills more Indians than any other single condition. It strikes earlier in the Indian population than in Western countries, often a decade sooner, driven by a combination of genetic susceptibility to dyslipidemia and insulin resistance, high rates of diabetes, rising rates of obesity and physical inactivity, tobacco use, and a diet increasingly influenced by processed food.
Yet the treatment available today — when coronary artery disease is detected early enough and managed by a skilled coronary artery disease specialist — is remarkably effective. Coronary angioplasty in heart arteries, supported by modern drug-eluting stents and evidence-based medication, gives patients with even severe coronary disease a very real path back to normal life.
The barrier is not treatment availability. It is awareness: patients who do not know the symptoms, who dismiss warning signs, or who do not understand what a coronary angioplasty and angiogram involve delay seeking help in ways that cost them heart muscle, cardiac function, and, sometimes, their lives.
This guide walks every reader through the complete pathway from recognizing symptoms through the diagnostic angiogram to PTCA stent placement and recovery—because understanding this pathway is genuinely life-saving.
Also read: Understanding PTCA Stent & Coronary Angioplasty expert
What Happens in Coronary Artery Disease
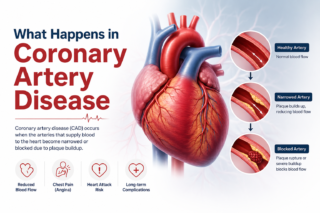
Coronary arteries are the three main blood vessels that supply oxygenated blood to the heart muscle itself. Coronary artery disease is the progressive accumulation of atherosclerotic plaque deposits of cholesterol, inflammatory cells, calcium, and connective tissue within the walls of these arteries. As plaques grow, they narrow the artery’s lumen, reducing the volume of blood the heart muscle receives.
In early disease, there are no symptoms. As narrowings become significant, the heart muscle receives adequate blood at rest but insufficient blood during exertion, producing the symptom of stable angina. When a plaque ruptures suddenly, as can happen without warning at any level of physical exertion, it triggers the formation of an acute blood clot that can completely block the artery, causing a heart attack
Heart attacks cause permanent heart muscle damage in proportion to the time the artery remains blocked. Opening the blocked artery within 90 minutes of symptom onset with emergency coronary angioplasty (primary PCI) salvages the most muscle and produces the best survival outcomes. Every minute matters.
Recognising the Symptoms: What to Know, and What to Take Seriously
Stable angina is exertional chest discomfort—a tightness, pressure, heaviness, or aching in the center of the chest that appears predictably during physical activity (walking uphill, climbing stairs, carrying loads) and relieves with rest within a few minutes. It may radiate to the left arm, jaw, or back.
In the Indian population, and particularly in patients with diabetes, coronary artery disease sometimes presents atypically without classic chest pain,but with unexplained breathlessness on exertion, unusual fatigue, or a feeling of heaviness or indigestion. These symptoms in any patient with cardiovascular risk factors deserve a prompt cardiac evaluation, not reassurance.
Acute coronary syndromes, unstable angina and heart attack, present with chest discomfort that is more severe and longer-lasting (more than 20 minutes) and may occur at rest. Associated symptoms, including sweating, nausea, breathlessness, or syncope, increase the likelihood of an acute event. These symptoms require immediate emergency care calling an ambulance and going directly to the nearest hospital capable of emergency coronary angioplasty in heart arteries.
The Diagnostic Pathway: From Symptom to Angiogram
The investigation of stable chest pain begins with clinical history, examination, a resting ECG, and blood tests. An echocardiogram assesses left ventricular function and wall motion. Stress testing exercises, ECG, stress echocardiogram, or nuclear perfusion imaging demonstrates whether coronary disease is causing ischemia during physical stress.
When an investigation suggests significant coronary artery disease, or when a patient presents with an acute coronary syndrome, coronary angiography is performed. This angioplasty and angiogram procedure takes 20 to 40 minutes under local anesthesia and sedation, with a catheter inserted through the radial artery in the wrist to deliver contrast dye into the coronary arteries while X-ray images map the distribution and severity of narrowings.
CT coronary angiography, a noninvasive alternative using CT scanning, is increasingly used as an initial anatomical investigation in stable patients with intermediate pretest probability of significant coronary disease, providing detailed arterial mapping without catheter insertion.
Also read: 5 Signs You or Your Elderly Parent May Need a Heart Valve Replacement
PTCA Stent: What the Procedure Involves Step by Step
When the angiogram reveals a narrowing that warrants treatment, angioplasty with PTCA stent deployment proceeds as follows:
A guidewire, a very thin, flexible wire, is advanced through the catheter and across the coronary narrowing. The wire serves as a rail for all subsequent equipment. A balloon catheter is advanced over the wire to the lesion site and inflated to compress the plaque, widening the arterial lumen. A drug-eluting stent coronary device, a metal mesh cylinder mounted on a second balloon, is then advanced to the same position and expanded, embedding itself in the artery wall and remaining in place permanently as a scaffold.
After stent deployment, the operator assesses the result using post-deployment balloon inflation to optimize expansion and intravascular imaging (IVUS or OCT) in many cases to confirm optimal stent apposition. Haemodynamic measurements confirm normal blood flow before all equipment is removed.
For heavily calcified lesions that require special preparation before stenting, chip angioplasty techniques, including intravascular lithotripsy or rotational atherectomy, are deployed to modify the calcium and allow adequate stent expansion.
The entire procedure for a straightforward single-vessel case typically takes 45 to 90 minutes.
Recovery: Life After a Coronary Stent
Recovery from coronary angioplasty is rapid compared to surgical alternatives. Most patients return to light daily activities within one to two weeks and to full activity within two to four weeks.
The most critical post-stent requirement is medication adherence. Dual antiplatelet therapy, aspirin combined with a second agent (clopidogrel, prasugrel, or ticagrelor), is prescribed for a defined period to prevent stent thrombosis. The duration depends on stent type and clinical risk profile. Stopping this medication early without medical guidance carries a risk of acute stent occlusion and must be avoided.
Long-term coronary artery disease management, statins, blood pressure treatment, diabetes optimization, and lifestyle modification continue indefinitely regardless of whether a stent has been placed. A stent treats the obstruction; it does not cure the underlying disease. Regular follow-up with the treating coronary artery disease doctor is essential for monitoring disease progression and adjusting treatment as needed.
Dr. C Raghu: Comprehensive Coronary Artery Disease Care in Hyderabad
Dr. C. Raghu coronary artery disease program in Hyderabad encompasses the full clinical pathway from initial risk assessment and non-invasive investigation through coronary angiography and complex coronary angioplasty to long-term secondary prevention management. His practice uses intravascular imaging and physiological assessment tools routinely, reflects current evidence-based guidelines in every decision, and provides clear, patient-centered communication throughout every stage of the diagnostic and treatment process.
For advanced coronary artery disease treatment, coronary angioplasty, and PTCA stent care in Hyderabad, consult Dr. C. Raghu at Yashoda Hospitals, Secunderabad — Call +91 95424 75650 today for expert cardiac care.
